Chronic Bronchitis: Understanding Cough, Sputum, and Quitting Strategies
If you wake up every morning feeling like you have to clear your throat before speaking, and that thick phlegm refuses to disappear after months of rest, you aren't just sick-you might be dealing with chronic bronchitis. Unlike a common cold that clears up in two weeks, this condition sticks around. It is clinically defined as a productive cough lasting at least three months for two consecutive years.
For many people, the constant cough and chest tightness become a background noise they try to ignore until it turns into breathing trouble. But understanding what's happening in your lungs is the first step toward taking control. While there is no magic cure, managing the disease effectively can significantly improve your daily life and longevity. The cornerstone of any recovery plan remains one undeniable truth: stopping smoking makes the biggest difference in slowing disease progression.
Why Does This Happen? The Basics of Airway Health
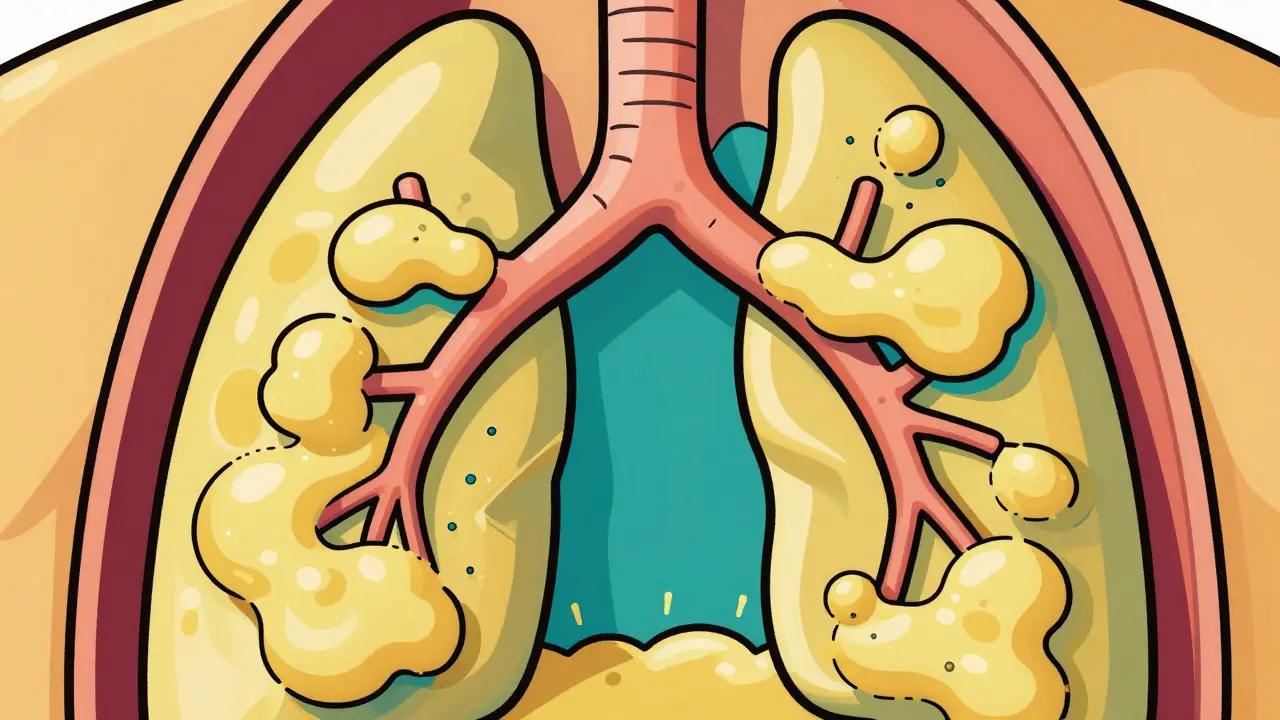
Chronic bronchitis is characterized by persistent inflammation and irritation of the bronchial tubes, leading to excessive mucus production. When healthy airways work, they stay clear and transport air efficiently. When you develop chronic bronchitis, the lining of those airways becomes inflamed and swollen. This swelling narrows the space air has to travel through.
Your body reacts to this irritation by producing more mucus, known as sputum. In healthy lungs, cilia (tiny hair-like structures) sweep this mucus away. In chronic bronchitis, these cilia are often damaged or paralyzed by smoke. The result is mucus pooling in the lungs, which triggers that relentless cough reflex trying to clear the blockage. About 75% of cases in the United States are directly linked to smoking history. Even among former smokers, the risk remains elevated compared to non-smokers, though quitting significantly slows further damage.
Symptoms Beyond the Cough
While the cough is the headline symptom, patients report a cluster of issues that affect energy levels and mobility. Shortness of breath is the most telling sign, especially during physical activity. According to clinical analyses, over 80% of patients experience significant breathlessness when exerting themselves, even for simple tasks like walking up a flight of stairs.
Other common signs include:
- Chest Tightness: Reported in nearly 70% of moderate to severe cases.
- Wheezing: A whistling sound when breathing, occurring in roughly 57% of patients.
- Fatigue: Nearly 3 out of 4 patients struggle with low energy due to reduced oxygen levels.
- Frequent Infections: Patients are 3.2 times more likely to develop viral or bacterial lung infections.
These symptoms typically begin appearing after age 40, with incidence rates climbing sharply past age 65. If you notice your stamina dropping faster than expected, or if you're getting sick more often than family members, it could signal underlying airway issues.
The Smoking Connection and Cessation Statistics
You cannot talk about chronic bronchitis without addressing tobacco. Over 90 percent of patients have a history of smoking. However, not everyone who smokes gets the disease-only about 15% of all cigarette smokers develop obstructive airway disease. This variability suggests genetics play a role, alongside environmental factors. Still, smoking remains the primary trigger. Long-term exposure to secondhand smoke contributes to 9% of cases among those who never smoked themselves.
Quitting smoking is not just advice; it is medical necessity. Studies show that patients who successfully quit smoking see disease progress 60% slower than those who continue. Furthermore, smoking cessation programs combined with behavioral counseling yield significantly better results than willpower alone. Structured programs incorporating varenicline or nicotine replacement therapy achieve abstinence rates around 45% at six months, compared to less than 7% for those attempting to quit without professional support.
| Method Type | Success Rate (6 Months) | Primary Mechanism |
|---|---|---|
| Unassisted Willpower | 7% | Behavioral determination |
| Nicotine Replacement Therapy (NRT) | 15% | Reduced cravings |
| Varenicline + Counseling | 45% | Neurotransmitter regulation + behavioral |
If you are struggling to find the strength to stop, remember that the average learning curve for adhering to medication regimens takes several sessions. It takes time to retrain your habits. Many patients find that integrated support groups help bridge the gap between knowing they need to quit and actually achieving it.

Treatment Protocols and Medication Options
Management focuses on relaxing the airways and reducing inflammation. Bronchodilators are the first line of defense. These medications relax muscles around the lungs, making it easier to breathe. Short-acting versions provide relief within 15 minutes but last only four to six hours. Long-acting bronchodilators are used for maintenance to keep airways open throughout the day.
Inhaled corticosteroids (ICS) are another option used for symptom relief, particularly in patients prone to frequent flare-ups. However, long-term use carries risks. Clinical guidelines note increased risks of osteoporosis, hypertension, and diabetes with prolonged steroid inhaler use. Doctors must weigh these side effects against the benefit of preventing exacerbations. Antibiotics are reserved for bacterial infections that worsen symptoms, with amoxicillin-clavulanate showing high efficacy for acute episodes.
| Medication Class | Primary Benefit | Major Risk/Side Effect |
|---|---|---|
| Beta-Agonists | Opens airways rapidly | Heart palpitations |
| Inhaled Corticosteroids | Reduces lung inflammation | Bone density loss (Osteoporosis) |
| Mucolytics (e.g., N-acetylcysteine) | Thins mucus | Gastrointestinal upset |
New treatments are also emerging. Recent advancements have approved phosphodiesterase inhibitors that reduce exacerbations without the heavy side effect profile of steroids. Additionally, vaccinations remain a critical part of care. Annual influenza vaccines reduce exacerbation risk by over 40%, while pneumococcal shots protect against pneumonia complications.
Pulmonary Rehabilitation: More Than Just Exercise
Many people think of rehab as just walking, but pulmonary rehabilitation is comprehensive education. It includes breathing techniques, nutrition counseling, and psychological support. Data shows these programs improve the distance patients can walk by an average of 78 meters in six minutes and reduce hospitalization rates by nearly 40%.
Why does this matter? Physical deconditioning sets off a vicious cycle. You get short of breath, so you move less. Moving less weakens muscles, making the next breath harder. Rehab breaks this cycle by safely conditioning your body to handle exertion again. Education on proper inhaler technique is also crucial here. Most patients require nearly five sessions with a respiratory therapist to master their devices correctly. Without this training, 38% of patients fail to receive full doses of their medication, essentially wasting expensive prescriptions.

Managing Your Daily Life
Daily management involves monitoring your own health trends. Pay attention to changes in the color or amount of your sputum. An increase in yellow or green phlegm often signals infection. Keep a record of your oxygen saturation levels at home if recommended. Oxygen therapy becomes necessary when blood oxygen drops below 88%. Continuous 24-hour oxygen use increases survival rates by 21% in patients with severe hypoxemia.
Avoid irritants beyond cigarettes. Household chemicals, dust from farming or construction, and outdoor air pollution contribute to about 30% of non-smoking cases. Simple steps like wearing a mask during cleaning or checking local air quality indices can reduce unnecessary stress on your lungs.
Looking Ahead: New Tools for Breath Control
As we move into 2026, the outlook continues to evolve. Digital health tools, such as smart inhalers that track usage, are proving to increase adherence significantly. Researchers are also exploring personalized therapies based on genetic markers related to mucus clearance. While we wait for these technologies to become widely available, sticking to current proven methods-quitting smoking, using prescribed medications consistently, and engaging in rehabilitation-remains the best strategy.
The goal isn't necessarily perfection, but progress. Whether that means walking down the street without stopping or simply sleeping through the night without coughing, every small improvement counts. Working closely with your healthcare team ensures you aren't navigating this condition in isolation.
Frequently Asked Questions
Can chronic bronchitis be cured completely?
Currently, there is no cure for chronic bronchitis once the damage is done. However, comprehensive management strategies can significantly improve quality of life, slow disease progression, and reduce the frequency of severe flare-ups.
Is smoking cessation effective if I've been smoking for decades?
Yes. Quitting smoking at any stage stops further damage. Studies indicate that quitting reduces the rate of lung function decline to near-normal levels, even after decades of smoking, drastically lowering the risk of respiratory failure.
What triggers a chronic bronchitis exacerbation?
Triggers include viral infections (like flu), bacterial infections, exposure to cold air, air pollution, and continued tobacco smoke exposure. Monitoring weather and air quality helps prevent unexpected flare-ups.
Does drinking water help clear the mucus?
Staying hydrated helps thin the mucus, making it easier to expel. However, hydration alone does not treat the underlying inflammation. It should be combined with mucolytic medications if prescribed by your doctor.
When should I start using oxygen therapy?
Oxygen therapy is typically started when blood oxygen saturation falls below 88% consistently. Long-term use can extend survival in severe cases and improves energy levels by ensuring your organs get enough oxygen.





Christopher Curcio
30 March, 2026 . 00:58 AM
The pathophysiology involves significant goblet cell hypertrophy throughout the tracheobronchial tree. We observe mucin hypersecretion as a primary defense mechanism against chronic irritation. Ciliated epithelial damage leads to impaired clearance of retained particulate matter. Consequently airway resistance increases significantly over repeated inflammatory cycles. Patients often underestimate the systemic impact of chronic hypoxemia on cardiac load. Cor pulmonale development is a serious long-term complication we must monitor closely. Pulmonary rehabilitation addresses the deconditioning aspect quite effectively in clinical trials. Nutritional support plays an underrated role in maintaining respiratory muscle mass during exacerbations. Pharmacological intervention should always prioritize bronchodilator efficacy before adding steroids. Inhaled corticosteroids carry bone density risks that require regular screening procedures. Varenicline shows superior outcomes compared to nicotine patches alone in cessation studies. Behavioral counseling bridges the gap between physiological dependence and psychological habit. Relapse rates remain high without sustained follow-up care after the initial quit attempt. Vaccination strategies targeting influenza and pneumococcus reduce hospitalization frequency considerably. Early detection of sputum color changes helps identify bacterial superinfection quickly. Proper inhaler technique remains critical for effective drug delivery in daily management.
Angel Ahumada
30 March, 2026 . 09:38 AM
the concept of society accepting chronic disease as inevitable speaks volumes about our cultural apathy towards self preservation why do we accept these limitations when biology fights back every time we breathe smoke we surrender autonomy over our own physiology
healthcare systems treat symptoms rather than root causes and this passive acceptance allows preventable suffering to continue unchecked the elite medical knowledge available remains inaccessible to those who suffer most from industrial pollutants we must demand better structural accountability
Kendell Callaway Mooney
31 March, 2026 . 09:46 AM
Pulmonary rehab is the missing piece for many patients managing this condition. Breathing techniques help control panic during breathlessness episodes. Walking programs build endurance slowly without causing excessive strain. Nutrition plans ensure patients maintain weight needed for breathing muscle strength. Psychological support prevents depression common with chronic illness diagnoses. Education on inhalers ensures medication actually reaches the lungs effectively.
dPhanen DhrubRaaj
2 April, 2026 . 07:04 AM
water helps thin mucus yes stay hydrated drink plenty of fluids helps clear airways faster
Calvin H
2 April, 2026 . 15:22 PM
Quit smoking already instead of reading about it.
Biraju Shah
3 April, 2026 . 08:25 AM
Willpower is not enough and telling people to just stop ignores the chemical dependency involved. Professional support and medication are necessary tools for breaking the addiction cycle. Ignoring this reality sets patients up for inevitable failure and worsening lung function.
RONALD FOWLER
4 April, 2026 . 03:18 AM
We need to support each other through the quitting process without judgment. Recovery looks different for everyone and patience is vital for progress. Small wins deserve recognition along the way.
Dan Stoof
5 April, 2026 . 15:10 PM
This outlook gives me such hope!! Science is advancing so fast and we finally have tools that work!!! Digital tracking is amazing!! Imagine smart inhalers telling us exactly when to use them!! We are going to crush this!!
Vikash Ranjan
6 April, 2026 . 06:27 AM
I am skeptical that technology alone solves behavioral issues. Many patients ignore gadgets despite knowing they exist. Personal responsibility outweighs tool availability in long term adherence.
William Rhodes
6 April, 2026 . 18:22 PM
True change begins with mindset shift toward valuing future health over immediate relief. Philosophy meets medicine when we understand life quality matters more than mere survival. Aggressive action now secures a better tomorrow.
Cameron Redic
7 April, 2026 . 17:21 PM
Mindset arguments ignore biological reality and enzyme deficiencies. Most relapse is driven by withdrawal symptoms not philosophy. Relying on vague motivation instead of proven medication leaves patients vulnerable to physical cravings.
Marwood Construction
9 April, 2026 . 06:00 AM
Clinical guidelines emphasize integrated care pathways combining pharmacotherapy with behavioral modification. Adherence protocols must be followed strictly for optimal outcomes. Regular pulmonary function testing provides objective metrics for treatment efficacy assessment.