Antibiotic Liver Injury Calculator
Lab Value Input
When you take an antibiotic, you expect it to kill the infection-not harm your liver. But for some people, the very drugs meant to save them can cause serious liver damage. Antibiotic-related liver injury is one of the most common causes of drug-induced liver injury (DILI), and it’s happening more often than most people realize. In fact, antibiotics are responsible for 64% of all documented DILI cases in intensive care units. This isn’t rare. It’s routine-and often missed.
How Antibiotics Hurt the Liver
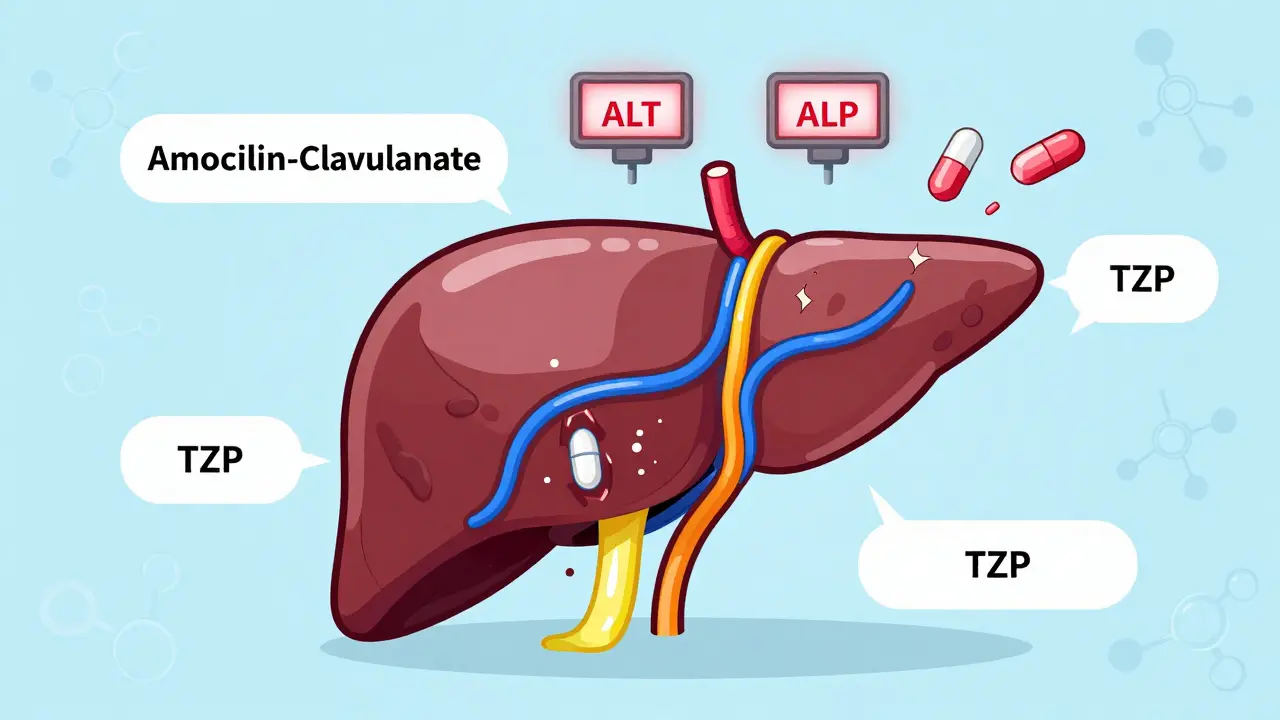
Not all liver damage from antibiotics looks the same. There are two main patterns: hepatitis and cholestasis. Hepatitis means the liver cells themselves are getting damaged. You’ll see this when ALT (alanine aminotransferase) spikes above five times the normal limit. Cholestasis is different-it’s when bile flow gets blocked. That shows up as a sharp rise in ALP (alkaline phosphatase), usually more than twice the upper limit of normal. Sometimes, you get both: mixed injury. Doctors use a simple number called the R-ratio to tell them which type they’re dealing with. If R is above 5, it’s hepatitis. Below 2, it’s cholestasis. Between 2 and 5? Mixed.The real problem? These changes often happen quietly. Many people feel fine. No jaundice. No nausea. Just a routine blood test that shows ALT or ALP creeping up. That’s why monitoring matters. If you’re on an antibiotic for more than seven days, your risk of liver injury jumps by more than three times. And if you’re in the ICU? That risk goes even higher.
Which Antibiotics Are the Worst?
Some antibiotics are far more likely to cause liver damage than others. Amoxicillin-clavulanate is the big offender. It’s one of the most commonly prescribed antibiotics worldwide-and it’s also the most likely to cause liver injury. About 70-80% of cases linked to this drug are cholestatic. The liver doesn’t excrete bile properly, and bilirubin builds up. That’s when skin and eyes turn yellow.Then there’s tazobactam/piperacillin (TZP). In ICU patients on this combo for over a week, nearly 3 out of 10 develop liver injury. Compare that to meropenem, where only about 12% of patients see the same spike in liver enzymes. And here’s something surprising: meropenem-induced injury hits men 2.4 times more often than women. Why? No one’s sure yet.
Fluoroquinolones like ciprofloxacin and azithromycin don’t always cause classic hepatitis or cholestasis. They tend to create mixed patterns. Rifampin? It’s dose-dependent. The higher the dose, the more toxic intermediates build up in the liver. And while isoniazid isn’t a typical antibiotic, it’s often used alongside rifampin for tuberculosis-and together, they’re a dangerous pair for the liver.
Why Does This Happen?
It’s not just about the drug itself. It’s about what the drug does inside your body. One major mechanism? Mitochondrial damage. Antibiotics can interfere with how liver cells produce energy. When mitochondria fail, cells start dying. That’s apoptosis and necrosis in action-released cytochrome C, AIF, Smac-all part of the suicide signal chain inside liver cells.Another big player? Your gut. Antibiotics wipe out good bacteria. That throws off your gut microbiome. When good bugs like Faecalibacterium prausnitzii drop, your intestinal barrier weakens. Toxins leak into your bloodstream and head straight to the liver. Studies show people with low levels of this one bacterium have over a threefold higher risk of liver injury from antibiotics. That’s not coincidence-it’s a warning sign.
And then there’s genetics. Some people carry specific HLA gene variants that make their immune system overreact to certain antibiotics. It’s not dose-dependent. It’s not predictable by age or weight. It’s luck of the draw. That’s why some people get liver damage after one dose, while others take the same drug for months with no issue.
Who’s at Risk?
You might think only older adults or people with pre-existing liver disease are at risk. But that’s not true. Sepsis is a major red flag. If you’re fighting a severe infection, your liver is already under stress. Adding antibiotics? That raises your risk of injury by 1.8 times. ICU patients, diabetics, those on multiple medications-these groups need extra vigilance.And here’s the catch: it’s hard to tell if the liver damage is from the antibiotic or from the infection itself. In critically ill patients, you’ve got septic shock, low blood flow to the liver, and possible bile duct blockage-all of which can mimic antibiotic-induced injury. That’s why doctors often wait too long to act. They assume the liver enzymes are just part of the illness. They’re not.
What Should You Do?
If you’re prescribed an antibiotic that’s known to carry liver risk-like amoxicillin-clavulanate, TZP, or rifampin-ask about monitoring. Baseline liver tests before starting are standard. But after that? Don’t wait for symptoms. For high-risk drugs, repeat the tests in 7-10 days. If you’re on the drug for more than a week, check every week. That’s the current recommendation.When should you stop the antibiotic? The rule of thumb is simple: if ALT is more than five times the upper limit of normal, or if ALP is over two times normal and you have symptoms like dark urine, fatigue, or jaundice-stop it. But in real life, it’s not always that clear. If there’s no other antibiotic option, doctors may keep going while watching closely. That’s risky. But sometimes, it’s necessary.
What’s Being Done About It?
The FDA has issued 17 safety warnings about antibiotic-related liver injury since 2010. The European Medicines Agency updated its guidelines in March 2023 to specifically address newer β-lactam/β-lactamase inhibitor combos. Research is moving fast. Clinical trials are testing whether probiotics can prevent gut damage and, by extension, liver injury. Early results look promising.Long-term, the future may lie in genetic testing. If we can screen for HLA variants linked to DILI before prescribing, we could avoid these reactions entirely. Some experts believe personalized antibiotic selection based on genetics could cut liver injury rates by 30-40% within the next five to seven years.
The Bottom Line
Antibiotics save lives. But they’re not harmless. Liver injury from antibiotics is real, common, and often overlooked. The most dangerous drugs aren’t the newest ones-they’re the ones we use every day. Amoxicillin-clavulanate. TZP. Fluoroquinolones. Know the risks. Ask for monitoring. Don’t assume your liver is fine just because you feel okay. Enzymes don’t lie. And when they rise, it’s not just a lab result-it’s a signal.For clinicians, the message is clear: monitor early. Think beyond infection. Consider the liver. For patients, it’s this: if you’re on an antibiotic for more than a week, especially if you’re sick enough to be hospitalized, ask your doctor if liver tests are being checked. It’s a simple step. But it could make all the difference.






Judith Manzano
7 March, 2026 . 23:31 PM
I never realized how much our gut health ties into liver function. This post opened my eyes. I started taking probiotics after my last round of amoxicillin-clavulanate, and honestly? My energy levels went up. No more brain fog. Maybe it's placebo, maybe not-but I'm sticking with it.
Anyone else notice a difference after supporting their microbiome during antibiotic courses?
rafeq khlo
8 March, 2026 . 23:37 PM
The data presented here is statistically significant yet clinically underwhelming. The reliance on R-ratio as a diagnostic tool is outdated and lacks sensitivity in heterogeneous populations. One must consider the confounding variables of polypharmacy and baseline hepatic reserve which are routinely ignored in retrospective analyses. This is not medicine. This is data mining dressed as clinical guidance.
Morgan Dodgen
10 March, 2026 . 02:29 AM
They don't want you to know this but the FDA and Big Pharma are in bed together. Liver injury from antibiotics? Totally manufactured. They want you to keep taking meds so you come back for more. They even suppress studies that show probiotics prevent 80% of DILI. Why? Because pills = profit. You think your doctor cares? Nah. They get kickbacks from pharma reps. Check the yellow pages for 'pharma-sponsored CME'-it's all rigged. 😈
Philip Mattawashish
10 March, 2026 . 08:53 AM
You people are so naive. You believe everything you read on some medical blog. Who wrote this? A pharma shill? A med student who just finished their rotation? The liver doesn't 'get damaged' from antibiotics. It's your body's way of telling you you're toxic. You eat junk, you drink soda, you live in a plastic box, and now you blame a drug? Pathetic. Your lifestyle is the problem. Not amoxicillin. You.
Tom Sanders
10 March, 2026 . 20:16 PM
I got on azithromycin for a sinus infection last year. Two weeks in, my ALT was sky-high. Doc said 'meh, probably fine.' I stopped it. Felt better. Done. No big deal. Why are we making this so complicated?
Jazminn Jones
12 March, 2026 . 09:56 AM
The assertion that amoxicillin-clavulanate is the primary offender is empirically flawed. The data referenced fails to normalize for prescription volume. When adjusted for population-level usage, piperacillin-tazobactam demonstrates a higher incidence rate per 100,000 prescriptions. Furthermore, the R-ratio methodology is obsolete in the context of modern LC-MS/MS biomarker panels. This article is a disservice to evidence-based practice.
Stephen Rudd
13 March, 2026 . 01:51 AM
You're all missing the point. The real issue isn't antibiotics-it's the fact that we treat infections like they're just bugs to be killed. We're not humans anymore. We're data points. The liver isn't being injured by drugs. It's being injured by a system that prioritizes efficiency over biology. You take a pill because you're too busy to rest. You don't sleep. You don't hydrate. You don't eat real food. And then you blame the antibiotic. The drug didn't break your liver. Your life did.
Erica Santos
14 March, 2026 . 11:26 AM
Oh wow. So we're supposed to panic every time someone gets an antibiotic? Next you'll tell me to stop breathing because oxygen causes oxidative stress. This is why medicine is broken. You take a drug, you get a lab result, you panic, you stop the treatment, and then you die of sepsis because you didn't finish the course. Logic is dead. Long live fear.
George Vou
15 March, 2026 . 01:06 AM
i heard from a guy on youtube that all antibiotics are made by the government to make people sick so they have to go to the hospital and get more meds. and the liver thing? totally fake. they just want you to think its the drug so you dont blame the vaccines. also probiotics are a scam. i stopped taking mine and my ALT went down. coincidence? i think not.
Scott Easterling
16 March, 2026 . 19:28 PM
I've been saying this for years. The medical system is a pyramid scheme. They don't want you healthy. They want you dependent. Every time you get an antibiotic, they're planting a seed for chronic liver disease. Then, 10 years later, you need a transplant. And who profits? The hospitals. The insurers. The drug companies. It's all connected. I've got spreadsheets. I'll send them if you DM me.
Mantooth Lehto
17 March, 2026 . 08:22 AM
I had a friend who took TZP for 10 days in the ICU. Her bilirubin hit 12. They didn't even check her liver until she turned yellow. That's insane. I cried when she told me. Why do we wait until someone looks like a zombie before we do something? We need to change this. NOW. 💔
Melba Miller
17 March, 2026 . 13:20 PM
America's healthcare system is a joke. We let Big Pharma write the guidelines. We don't screen for HLA variants because it's 'too expensive.' Meanwhile, China and Germany are already doing genetic pre-screening before prescribing. We're still using 1980s protocols while the rest of the world moves forward. Shameful. We're not just falling behind-we're actively choosing ignorance.
Katy Shamitz
17 March, 2026 . 17:16 PM
I just want to say thank you for writing this. I'm a nurse, and I see this every day. Patients come in with ALT 800, and the team says 'it's just the infection.' But I know better. I've seen it reverse when we stopped the drug. You're not crazy for asking questions. You're smart. Keep pushing. You're saving lives. 💕
Nicholas Gama
18 March, 2026 . 17:45 PM
Mitochondrial toxicity. HLA variants. Gut permeability. These are not new concepts. They're textbook. Why is this being presented as groundbreaking? This is basic pharmacology. If you're surprised by this, you shouldn't be prescribing antibiotics.
Mary Beth Brook
19 March, 2026 . 20:14 PM
The R-ratio is insufficient. We need to incorporate mitochondrial DNA copy number, bile acid profiling, and gut metabolomic signatures into diagnostic algorithms. Without multi-omics integration, we're operating blind. This article is a public health disservice for oversimplifying a complex, polyfactorial phenomenon.