
Serotonin Syndrome Assessment Tool
This tool helps you quickly assess potential serotonin syndrome symptoms based on clinical criteria. If you or someone you know is showing signs of serotonin syndrome, stop all serotonergic medications immediately and seek emergency care.
What Is SSRI-Induced Serotonin Syndrome?
SSRI-induced serotonin syndrome isn’t a rare side effect-it’s a medical emergency that can turn mild discomfort into life-threatening chaos in just hours. It happens when too much serotonin builds up in your brain, usually because you’re taking more than one medication that boosts serotonin levels. SSRIs like sertraline, fluoxetine, or escitalopram are common triggers, especially when mixed with other drugs like tramadol, migraine meds (triptans), or even certain herbal supplements like St. John’s wort.
This isn’t about feeling a little ‘wired.’ It’s about your nervous system going into overdrive. The body’s serotonin receptors get flooded, and your muscles, heart, and mind start acting out of sync. About 67% of people who develop this condition show symptoms within six hours of a new drug, a dose increase, or an interaction. And here’s the scary part: nearly half of emergency room staff miss the diagnosis the first time.
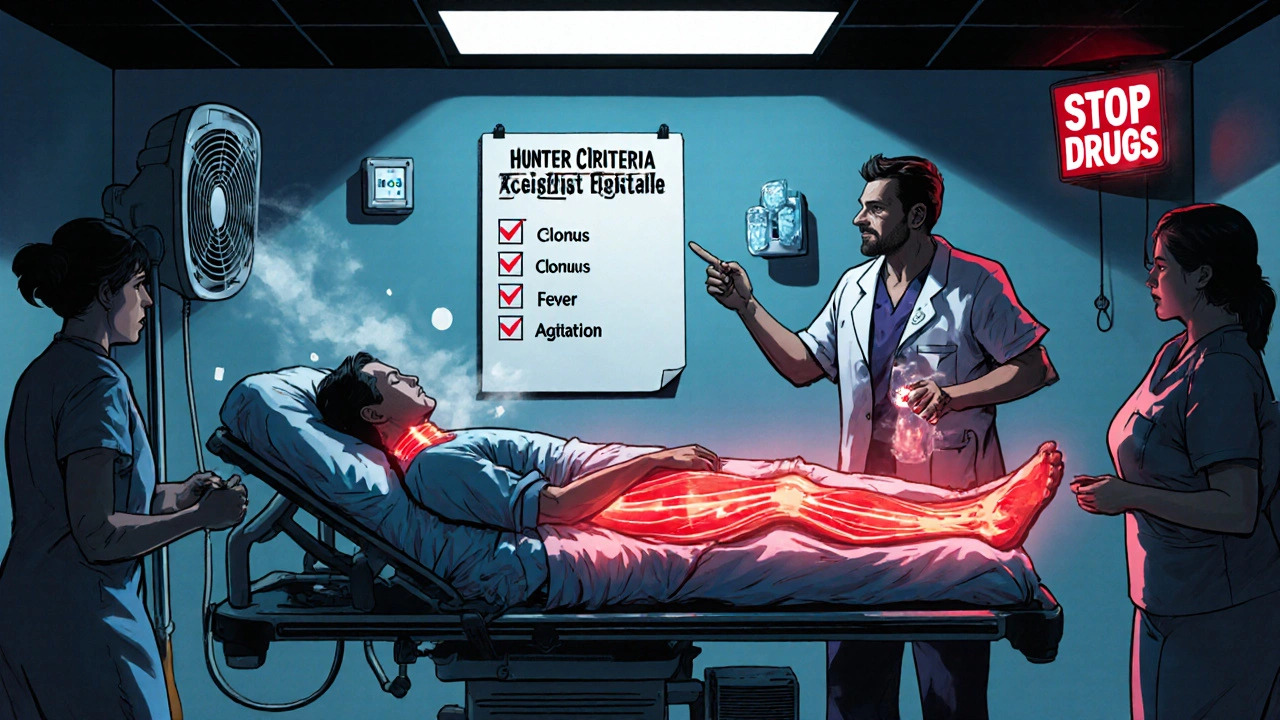
The Three Signs You Can’t Ignore
If you’re on an SSRI and suddenly feel off, look for these three patterns together. One alone might be something else. All three? That’s serotonin syndrome.
- Cognitive changes: Agitation, confusion, racing thoughts, hallucinations. You might feel like you’re losing control of your mind.
- Neuromuscular signs: Clonus (involuntary muscle spasms), tremors, rigid muscles, overactive reflexes. Ocular clonus-when your eyes jerk uncontrollably-is a red flag doctors look for.
- Autonomic chaos: Sweating so heavy your clothes soak through, heart rate over 120, high or low blood pressure, fever above 38.5°C (101.3°F), diarrhea.
These aren’t random symptoms. They’re a direct result of serotonin overload. The Hunter Serotonin Toxicity Criteria, used in hospitals worldwide, confirms the diagnosis when you have clonus plus one other sign-like agitation or fever. It’s 84% accurate. If you see this combo, don’t wait.
Severity Levels: Mild, Moderate, Severe
Not all cases are the same. The difference between a bad day and a hospital stay comes down to temperature and muscle rigidity.
- Mild: Temperature under 38.5°C (101.3°F), symptoms in one or two categories. You might feel anxious, sweaty, and shaky-but still able to walk and talk.
- Moderate: Temperature between 38.5°C and 41.1°C (101.3°F-106°F), all three symptom groups present. You may be confused, unable to stand without help, and your muscles feel locked.
- Severe: Temperature over 41.1°C (106°F), severe muscle rigidity, seizures, organ stress. This is critical. Your body is overheating from muscle activity, not infection. And yes, it can kill.
Here’s what most people don’t realize: mild cases can crash into severe within four to six hours. A 2022 study found 43% of ER doctors didn’t know this. If you’re on an SSRI and feel worse after starting a new medication, assume it’s serotonin syndrome until proven otherwise.
What to Do Right Now: Emergency Response
Time is everything. The faster you act, the better your odds.
- Stop all serotonergic drugs immediately. This includes your SSRI, tramadol, migraine pills, dextromethorphan (in cough syrup), or even supplements like 5-HTP. Don’t wait for a doctor’s call.
- Call 911 or go to the ER. This is not a home remedy situation. Even mild cases need monitoring.
- Do NOT use acetaminophen or ibuprofen for fever. These won’t help. Your fever isn’t from an infection-it’s from muscles shaking nonstop. Cooling your body externally is the only way.
- Stay calm. Avoid physical restraints. Holding someone down makes muscle spasms worse, raising body temperature further. Let trained staff handle it.
In the ER, the first-line treatment is benzodiazepines-diazepam or lorazepam. They calm your nerves, relax muscles, and prevent seizures. For moderate cases, cooling with fans and misting works. For severe cases, doctors may intubate you, paralyze your muscles with rocuronium, and use ice packs on your neck, armpits, and groin. In 2024, a major trial showed adding dantrolene (a muscle relaxant) cut death rates in half for the worst cases.
Why Cyproheptadine Is Controversial
You might hear about cyproheptadine-an antihistamine that blocks serotonin receptors. It’s sometimes given as 12mg initially, then 2mg every two hours. But here’s the truth: there’s no strong clinical trial proving it saves lives. Most evidence comes from case reports. It’s used when benzodiazepines aren’t enough, but it’s not a magic bullet. In fact, some hospitals don’t stock it at all. Don’t rely on it. Focus on stopping the drugs and cooling the body.
What Doesn’t Work (And Why)
Many well-meaning people try the wrong things-and it makes things worse.
- Antipyretics (Tylenol, Advil): Useless. Fever isn’t regulated by your brain’s thermostat-it’s from muscle contractions.
- Physical restraints: Increase metabolic demand. More muscle activity = more heat = faster decline.
- Waiting to see if it gets better: 78% of emergency physicians underestimate how fast this progresses. A case can go from mild to life-threatening in under six hours.
- Continuing the SSRI: Even if you think it’s just anxiety. That’s what one Reddit user did-kept taking sertraline after adding tramadol. Within four hours, she couldn’t walk, had a heart rate of 130, and ended up in ICU.
Who’s at Highest Risk?
It’s not just about taking SSRIs. It’s about combinations.
- SSRI + MAOI: 12.4 times higher risk. This combo is deadly. Never mix them.
- SSRI + tramadol: 8.7 times higher risk. Tramadol is in many pain meds-even over-the-counter ones in some countries.
- SSRI + triptans: 3.2 times higher risk. Common migraine treatments like sumatriptan.
- SSRI + St. John’s wort or 5-HTP: These herbal supplements aren’t regulated. Many people don’t realize they’re serotonergic.
Fluoxetine (Prozac) is especially tricky. Its active metabolite sticks around for weeks. Even after you stop it, serotonin levels stay high. Recovery can take 3-4 weeks. Other SSRIs clear faster.

Real Stories: What Happens When It’s Missed
A woman on the Anxiety and Depression Association of America forum was told she was having an ‘anxiety attack’ while her temperature hit 39.4°C and her eyes were jerking uncontrollably. She waited eight hours before someone recognized ocular clonus. By then, she needed ICU care.
Another man started a new SSRI, then took a cold medicine with dextromethorphan. Within hours, he couldn’t speak clearly, his legs were rigid, and his skin was hot to the touch. His family didn’t know what was wrong. He was misdiagnosed with a stroke. He survived-but barely.
Early recognition saves lives. 92% of mild-to-moderate cases resolve within 72 hours if the drugs are stopped. But if treatment is delayed more than six hours, death risk jumps from 2% to over 11%.
What Hospitals Are Doing Now
Some ERs have started using standardized protocols. One study across 15 U.S. hospitals found that after implementing checklists and staff training, time-to-treatment dropped from 112 minutes to 37 minutes. That’s the difference between recovery and tragedy.
Starting in January 2025, the Joint Commission will require all emergency departments to train staff on serotonin syndrome recognition. That’s a big step. But until then, you have to be your own advocate.
What You Can Do Today
- Know your meds. Keep a list of everything you take-prescription, OTC, supplements.
- Check for interactions. Apps like ‘Serotonin Alert’ can scan your meds and flag risks (92% accurate, per 2023 study).
- Teach someone close to you the signs. If you’re alone when it hits, they need to know what to look for.
- If you’re starting a new drug while on an SSRI, watch for symptoms the first 24 hours. That’s when it’s most likely to happen.
Recovery and Aftercare
Most people recover fully if treated early. But you can’t just jump back on your SSRI. Wait at least two weeks after symptoms clear, and only restart under a doctor’s supervision. Some patients need to switch to a non-SSRI antidepressant like bupropion, which doesn’t affect serotonin.
Long-term, keep a record of this episode. Future doctors need to know. And if you’re prescribed any new drug-even for pain or sleep-ask: ‘Is this safe with SSRIs?’
Can serotonin syndrome happen from one SSRI alone?
Yes, but it’s rare. Most cases happen when an SSRI is combined with another serotonergic drug. However, high doses of SSRIs-especially fluoxetine or paroxetine-can cause it on their own, particularly if the dose was increased too quickly.
How long does serotonin syndrome last?
Mild cases usually resolve in 24-72 hours after stopping the triggering drug. Moderate cases may take up to five days. Severe cases can last a week or more, especially if the drug has a long half-life like fluoxetine, which can linger for weeks.
Is serotonin syndrome the same as neuroleptic malignant syndrome?
No. Neuroleptic malignant syndrome is caused by antipsychotic drugs, develops over days, and causes ‘lead-pipe’ muscle rigidity without clonus or hyperreflexia. Serotonin syndrome comes on fast, involves clonus, and is linked to SSRIs or other serotonin boosters.
Can I take SSRIs again after having serotonin syndrome?
It’s possible, but risky. Only restart under close medical supervision, and usually with a different class of antidepressant. Never restart the same SSRI or combine it with other serotonergic drugs again.
Are there any long-term effects of serotonin syndrome?
Most people recover fully without lasting damage. But severe cases that caused prolonged high fever or seizures can lead to muscle damage, kidney issues, or nerve problems. Early treatment prevents this.




Malia Blom
8 November, 2025 . 01:13 AM
So let me get this straight-you’re telling me the entire medical establishment is just winging it on serotonin syndrome? Like, 43% of ER docs don’t even know mild can turn severe in 6 hours? That’s not incompetence, that’s systemic neglect. We’ve turned healthcare into a click-driven hustle and now people are dying because no one’s got time to learn the difference between anxiety and clonus. 🤷♀️
Erika Puhan
8 November, 2025 . 09:51 AM
The pharmacokinetic profiles of SSRIs are not merely "complex"-they are fundamentally incompatible with the neoliberal imperative of rapid, self-managed pharmaceutical intervention. The conflation of symptomology with consumer autonomy is a bioethical failure of epistemological magnitude. You cannot "just stop" a drug with a half-life of 7-9 days and expect homeostasis. This is not a checklist-it’s a metaphysical crisis.
Edward Weaver
9 November, 2025 . 16:13 PM
I’ve seen this happen in the VA. Guy takes tramadol for back pain, keeps his Zoloft, and suddenly he’s screaming in the waiting room with eyes jumping like a glitchy screen. We got him cooled down, gave him 10mg lorazepam, and he was lucid in 20 minutes. If you’re not in the US and you think "herbal supplements" are safe, you’re living in a fantasy. We don’t regulate that crap here because we’re not a socialist dystopia. You want safety? Take responsibility.
Lexi Brinkley
11 November, 2025 . 13:58 PM
OMG I JUST SAW THIS AND MY BESTIE IS ON SSRIS AND TOOK TRAMADOL FOR HER MIGRAINE 😱😭 I JUST TEXTED HER TO STOP EVERYTHING AND GO TO THE ER 💪💉 I’M SO GLAD I READ THIS THANK YOU 🙏❤️
Kelsey Veg
13 November, 2025 . 07:16 AM
ok so like i was on lexapro and took some cough syrup with dextro and felt weird for a sec but then it passed so i thought it was just stress?? like wtf why is everyone making this sound so apocalyptic?? i mean i lived??
Alex Harrison
14 November, 2025 . 18:50 PM
I think this post is super important but I have to say I didn’t know about the dantrolene thing-sounds like it could be a game changer. I’m a nurse and we’ve been using benzos and cooling for years, but I’ve never seen it in action. I’ll bring this up at rounds tomorrow. Also, typo: "serotonergic" is spelled right but I keep missing the "g" when typing fast. 😅
Jay Wallace
15 November, 2025 . 01:51 AM
Let’s be real: if you’re taking St. John’s Wort with an SSRI, you’re not "self-medicating"-you’re playing Russian roulette with your brainstem. And don’t get me started on the "natural remedies" cultists who think their tea is safer than FDA-approved meds. You don’t get to opt out of pharmacology because you watched a YouTube video. This isn’t a lifestyle choice-it’s a biological reality. And yes, I’m calling out the hippies.
Alyssa Fisher
16 November, 2025 . 02:01 AM
There’s something deeply human about how we treat medical emergencies like puzzles to be solved by checklist rather than experiences to be witnessed. Serotonin syndrome isn’t just a list of symptoms-it’s the body screaming that its chemistry has been hijacked. We’ve built a system that rewards speed over presence, and that’s why people die waiting. The real solution isn’t just better training-it’s relearning how to listen. To the patient. To the tremor. To the eyes that won’t stop moving. That’s where the diagnosis begins-not in the algorithm, but in the silence between the symptoms.